 Your law firm is a business; and running a successful business is HARD. There are myriad books, websites, and seminars dedicated to how to run your business, but there are some common threads. According to Forbes Magazine one of the most important steps you can take to run a successful business is to optimize your efficiency by outsourcing what you can.[i] Not a social media guru? Hire a virtual social media pro. Struggle with keeping track of costs? Hire an accountant or bookkeeper. Unfamiliar with medical lingo, the structure of EMRs, and the standard of care? Hire a medical professional to consult with you. A medical professional can greatly reduce the amount of time spent reviewing medical records just by virtue of understanding the structure and content of medical records on a fundamental level. Medical jargon can be as intimidating as another language and understanding the implications of different procedures, items in a medical history, and medications requires literally years of concentrated study and clinical experience- you don’t have time for that! So, “bring in the professionals!” recommends Business News Daily.[ii] A Legal Nurse Consultant is just that- a medical professional with legal knowledge and/or training who can help distill the most pertinent and relevant facts of the case into various reports to help keep your cases moving.
|
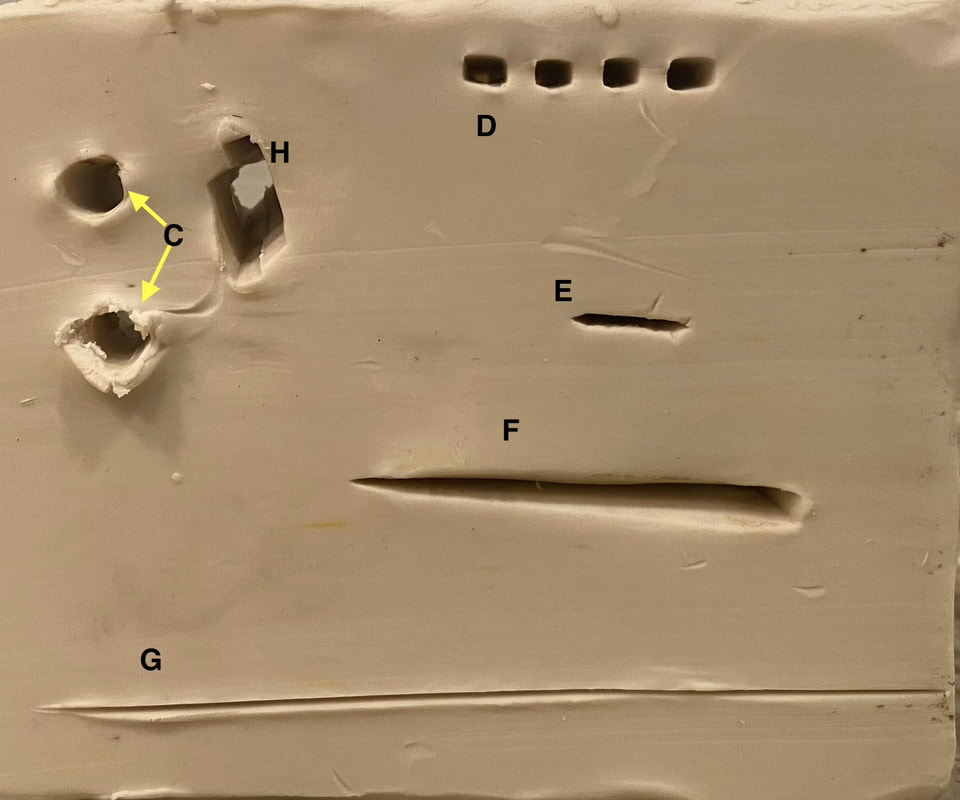 |  |

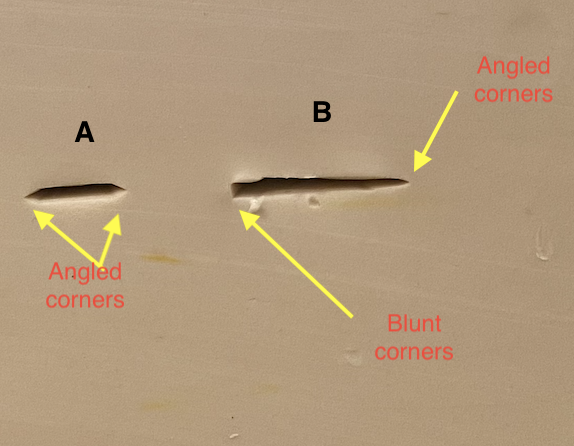
Types and Causes of Blunt Force Trauma
Blunt force trauma happens when a part of the body strikes, or is struck by, a blunt object. Generally speaking, blunt objects that cause injury have much greater surface area relative to sharp objects that cause injury. With sharp-force trauma (detailed blog post is in the works) the cutting edge only needs a small surface area to cause injury. Common objects causing blunt force trauma include vehicles, fists, sidewalks, roads, baseball bats, and hammers. Common blunt-force injuries include abrasions, avulsions, contusions, & lacerations.
Abrasions
Abrasions occur when a part of the body scrapes across another surface, generating enough friction to disrupt skin integrity. Sometimes the skin and the surface causing the abrasion come into contact briefly (think of the accidentally scraping your upper arm against a brick wall, or falling onto your outstretched hand) and other times the contact with the surface can be prolonged (such as that of a body being dragged underneath a car and scraping against the road).
Abrasions can happen due to the skin having contact with either a hard or a soft surface, although obviously more force would be needed to cause an abrasion with a soft surface. The examples above describe the contact of skin with a hard surface. An example of a soft surface causing an abrasion would be ligature marks on the wrists of someone restrained with a shoelace.
The direction in which the force was applied can be determined by which part of the wound margin demonstrates more skin “beading.” The last part of the wound to have contact with the offending surface will show more skin beading that the rest. In the photo, the skin beading visible on the left-most aspect of the wound margin (red arrow) indicates that the direction of force likely followed the direction of the black arrows. Beaded skin sloughs off soon after injury so early photos of injuries are key.
Matter embedded in an abrasion or laceration can also help determine mechanism of injury. For example tiny, cube-shaped fragments of glass in an abrasion following a motor vehicle accident indicate the glass was from a side-window (made of tempered glass) rather than a windshield (made of laminated glass, which shatters into longer, flatter shards). This can help determine an individual is being truthful about their position in the vehicle during a motor vehicle accident case.
Click read more (below box to right) to continue.

The first thing to consider is what you want the Legal Nurse Consultant (LNC) to accomplish. Have you already accepted this case? Or are you considering taking a case and you want the LNC to review for merit?
An LNC may be able to give you an estimate for a merit review based on information you can provide over the phone before you even send the medical records. They will need certain information, however, including number of pages & type of medical records (100 pages of hospital records is way different than 100 pages of psychotherapy records). He or she may also want to know what you- as the attorney- view as the strengths and weakness of the case, as well as what the allegations are.
If you’ve already accepted the case, the LNC will need the above information and will also evaluate what your needs are: what services can they provide you? Are you looking for a timeline? Gantt chart? Demonstrative evidence? A chronology? An expert witness? The LNC can explain what services they offer and tailor them to meet your needs.
It’s important to make the LNC aware of the expected date of mediation or trial and any other deadlines you may have. He or she will also want to know how the medical records will be received (through ShareFile, DropBox, physical copies, thumb drive etc). Inform your LNC if you have a set budget for LNC services. Many LNCs prefer to work on a retainer basis in order to guarantee check-ins with the attorney to make sure the attorney is satisfied with the work being done.
To avoid miscommunication you should provide the Legal Nurse Consultant with the contact information for their primary point of contact in your office- will he be hearing from a paralegal by phone? From a case manager by email?
Finally, you should let the LNC know up front if you have any specific preferences in the formatting of your work product. Many attorneys have preferences with regard to font size, typeface, whether documents should be Bates stamped, etc. While they’ll be happy to make changes for you if you don’t realize a preference until later, if you already know what your preferences are, go ahead and let us know! If you have any questions regarding services, fees, or anything else it’s always a good idea to write them down before your call.
If you’re ready to organize, streamline and clarify the medical records associated with your legal case, get in touch with us today for a free thirty minute phone consultation!
 | |

Determining what the standard of care is in a case is frustrating because even the phrase, “standard of care” sounds finite. Using the word “standard” conjures ideas of benchmarks, tests, and objectively measurable data. Life would certainly be easier for the legal (and to be honest, the medical) community if defining a standard of care were so easy, but it's not.
The medical practitioner’s duty to the patient is not determined simply by checking boxes in a list of symptoms. It is individual & determined by the specific circumstances of the specific patient (with a unique history) experiencing specific symptoms in a certain place & time. It also must take into account the resources available to the practitioner. An internal medicine doctor practicing in small primary care office in rural Georgia can’t be held to the same standards regarding what laboratory or imaging tests can be run in-house as an internal medicine doctor practicing in a large tertiary referral center. It boils down to the duty of the medical practitioner to know (& put into practice) those medical decisions which any other (“reasonable & prudent”) practitioner would make given the same patient in the same circumstances. That’s why expert physician witnesses are always going to be your best bet when it comes to defining the standard of care on the witness stand (for physicians; you would need a nurse expert witness for the nursing standard of care, etc).

Legal Nurse Consultants can help with a wide variety of cases, their scope is not limited merely to medical malpractice. Many offer free consultations, so reach out to an LNC today for help with any case involving medical records or medical history, including
or defense, personal injury & more.
If you are wondering whether a Legal Nurse Consultant can help with your case, contact us today for a free 30-minute phone consultation to discuss your case.
7/7/2021 0 Comments
What's An Attorney to do When Confronted with the Possibility of Altered Medical Records? (Part 4/4)

When you send a medical records request to a facility what you are going to get is essentially a printed-out version (or, this day and age probably a PDF of how it would look printed out) of the notes entered about the patient while they were in the hospital as they would appear in the computer system if you were to open up the chart at the facility- which is great, right?
Not necessarily. In this case you are seeing the medical record as the providers and the facility want you to see it.
It could be unchanged from its original state, but since the provider doesn’t have to scratch out their incorrect entries you will not be able to tell when the entries were truly made (despite the time stamp) or whether any entries were deleted or modified. Having slightly late entries is not uncommon and is not necessarily an indication of fraud. In fact, most of the time unless the health care provider is working with a scribe (which is actually becoming pretty common in some settings) they are going to have to document what happens during a patient encounter after-the-fact. Think of it this way, you wouldn’t come out of the room after deposing a client with deposition digest already in hand. You have to review the deposition and complete process it when you’ve had time to think. However one thing the EMR allows providers to do is to edit, delete and add-in entries days, months and even years later but date them for the time of the patient contact. The problem is that in your typical medical records request, that late entry is going to look like it was entered at the time that the patient encounter occurred (if that’s how the person entering the entry wants it to look). It’s very easy to “back-date” an entry so that it looks like something was documented in a timely fashion when it may not have been.
There are federal laws dictating the types of technical safeguards that must be in place for an EMR so that late entries and tampering can be detected (The Cures Act Update 45 CFR § 164.312, HIPAA, HITECH and more). EMRs must have a method of tracking who accesses a medical record, when the medical record was accessed, the terminal or location the medical record was accessed from and what the person accessing it did- including whether they entered, modified or removed data. This is referred to as an audit log or audit trail.
The audit log is basically a timeline that states the name, time, location, and method of access of every person who opened the patient’s electronic medical record. Even if the person who opened it made no change to medical record- didn’t write a note, chart a vital sign, nothing- their name and other pertinent information will show up on the audit log.
The downside to this is you can have a ton of data that translates to very little usable info. Most of the time you won't want to request the audit log for all of the patient's records. You can specifically request an audit log specific to certain dates, for example; or an audit log showing certain actions or all actions taken by a specific provider.
The big take-away here is that the metadata (commonly described as "data about data") available in an audit log is not considered a part of the patient’s medical record. Obtaining the audit trail requires a separate discovery request; but unless you want to scale a mountain of medical records, make your discovery request very specific.
If you request an audit log and you see a lot of modifications (especially if those modification took place much later or after your legal team originally requested access to medical record) there is yet another step you may need to take.
If you have significant reason to believe a record has been tampered with you can also request a revision history. The revision history shows all available versions of a chart, so someone analyzing it can tell what the chart said before a modification was made and what it said afterward. An easy way to think of the revision history is to think about using the “Track Changes” function in Microsoft word. It is a list in chronological order showing the different versions of what has been changed and when. It’s a ton of documentation and will result in an extra cost and time burden if requested, but could be priceless if significant alterations are discovered.
Check out part 1 (Missing and Altered Medical Records: the Value of a Clinical Eye on Deficiencies in Medical Records), part 2 (Why do Parts of the Medical Record Go Missing?) and part 3 (What's an Attorney to Do Regarding Missing Medical Records?) in this series for more information.
To get the most comprehensive and up-to-date information about identifying and handling challenges associated with missing and altered medical records, submit an inquiry below or visit our CLE page.
When trying to identify missing medical records and overcome the barriers associated with missing records, clinical and practical understandings of hospital policies and the standard of care are so important. This a huge area of opportunity for Legal Nurse Consultants to really shine. A nurse who has been in the trenches working with patients will know what tests this patient should have had and will be able to recognize when they are missing. He or she will know what documentation should be present in a variety of clinical situations and may be able to help formulate record requests to help you get exactly what you need.
Shameless plug- Obviously as a legal nurse consultant and business owner who believes in the value of what I do, I’m going to tell you that I, or someone like me, is going to be your best resource for identifying deficiencies in the medical record. As someone who has had to document in a chart and audit charts of my peers I know how to look for what’s missing in documentation. Working as a nurse, this was self-preservation- I needed to my sure there weren’t deficiencies in my documentation so that I was covered if something went wrong.
But if you still aren’t ready to work with a legal nurse consultant, here are a few tips to get you started on your own:
- Organize the record chronologically with an index. This just makes sense. In an ideal situation you have electronic copies of all records, in chronological order with an index or table of contents that is hyperlinked so that you can click on the name of a record from the table of contents and be taken there. This is a service some LNCs provide (including myself).
- Compare billing records to medical records- Are there tests or procedures that were billed for that you don’t see reflected in the medical record? Is there bill for wound care but you don’t see a note from a Wound Care Nurse? Do you see a bill for a blood transfusion but no signed consent and no documentation about the transfusion?
- Create a Treater List: A treater list is exactly what it sounds like- a list of the name of every single health care provider or facility (including imaging centers and pharmacies) mentioned in the medical record. Did the ER doctor state in a note that she referred the patient to the Neurologist Dr. Billings? Put Dr. Billings’ name on the treater list so you can make sure you have his notes. Did the doctor write in a note that, “the patient stated she was previously seen two weeks ago at Methodist Hospital”? Write “Methodist Hospital” on the treater list and make sure you have records from that hospital.

This was a long post, but I hope it helps you overcome some of the difficulties associated with identifying and obtaining missing pieces of the medical record. Although this post mostly dealt with things that are left out by accident, Part 4 of this Four-Part series on Missing and Altered Medical Records will deal with records that have been intentionally altered. It will be up soon!
What other issues have you come up with when medical records are missing? Comment below!
Other parts of this series:
Part I Introduction
Part II Why Do Parts of The Medical Record Go Missing?
It’s obvious that having incomplete medical records on hand can break your case, so why are incomplete medical records so common? It's important to note that in most cases in which portions of the medical record appear to be missing there is likely a reason for it that doesn't involve fraud, but that doesn't make your situation as the attorney receiving the records any easier.
Since the implementation of Electronic Medical Records (EMRs) in the vast majority of health care facilities, one would think it would be easy to just print the whole record out (or- more likely these days- save everything as one PDF) and have everything at your fingertips. Unfortunately that isn’t always the case. In the rush to become compliant with the Patient Protection and Affordable Care Act (PPACA), HITECH and other information systems legislation of the early 2000s implementation of a comprehensive and purely electronic medical record is still something we’re only dreaming of.
One huge barrier to a comprehensive medical record is that people have a tendency to go doctor shopping. If they go to one doctor and don’t like the diagnosis or proposed plan of care they just switch to a new doctor. In many cases they don’t even keep track of which doctors they’ve been to for what condition. In my experience as an ER nurse we would even get patients who would go to one ER and not like what they heard and then go stand across the street from the hospital they just left and call 911 for an ambulance ride to another hospital to try and get a “second opinion.”

Unfortunately the answer is “probably not,” and there are several reasons why this might happen.
Point-of-Care labs and other tests. Point-of-Care tests are tests done at the bedside with the patient. One of the most common is blood glucose in people being monitored for diabetes but heart enzymes, certain urine tests, EKGs and others can be done at the bedside as well. Sometimes the nurse gets the result as a read-out on the screen and sometimes there’s a print out that will supposedly get scanned into the medical record eventually. Some companies have come up with ways to interface their point of
Other labs must be sent off for testing. Send off tests can be incredibly frustrating for the healthcare provider. Unfortunately most- if not all- hospital labs don’t have the capability to keep the equipment and supplies needed for 100% of the tests that might be ordered on a patient on site. You may remember that in the earliest days of the Covid 19 pandemic there were many hospitals and offices that had to send their specimens off to the CDC and wait days for results. This happens with a lot of other types of tests too. This can lead to the results not getting entered into the patient record in a timely fashion or to the results being entered in an incorrect part of the medical record, especially if the patient is discharged from the facility or transferred to another part of the hospital before the results come in.
Imaging done at other facilities. This wouldn’t apply in the case of Ms. Mabel because she is the one patient in the world who gets everything done in one place, but for many real patients this is the case. The patient may go to any number of outpatient facilities for MRIs, CT scans, ultrasounds etc and then a radiologist (who may even be working remotely out-of- state) reads the scans and makes the report. Now the physical image is one place, the report is coming from another and we just have to hope both make it back to the patient’s chart without getting separated.
Jumbled records. Even when all of the records come from one facility they may not have been printed or bound in order. Many EMRs have slightly different charting systems for different departments (such as ER, radiology etc) and the person compiling the medical record may not have the ability or inclination to streamline them for you.
There are plenty of other reasons you may be missing significant parts of the your client’s medical records, but it’s time to get to meat of the matter- What’s an attorney to do? I cover that in part three (coming soon).
5/13/2021 3 Comments
Missing and Altered Medical Records: The Value of a Clinical Eye on Deficiencies in Medical Records (Part 1 of 4)

Nurses have background knowledge of-
- How frequently vital signs should be checked on different types of hospital wards based on acuity
- Which procedures (including “Code Blue”/Resuscitations) have additional flowsheets that may not have been a part of the electronic medical records
- Which seemingly routine procedures (such as blood transfusions, applying a splint to a broken arm) may require additional consent forms which may not be present in the electronic medical record
- Which patient care situations include incident reports that are kept internally and not considered a part of the patient’s medical record at all. This may include things such as how a patient fall or needle stick injury was handled.

When a legal professional is reading through medical records and pathology reports they can get bogged down in doing research about abrasion- vs avulsion- injuries: how are they differentiated? What aspects do they have in common? What mechanisms of injury can cause an avulsion? What mechanisms of injury cause abrasions? Is there any crossover? And most importantly: Does how the plaintiff says the injury happened track with how the injury looks or is described in the medical record?
 Avulsion |  Abrasion |
Archives
February 2022
October 2021
September 2021
August 2021
July 2021
June 2021
May 2021
April 2021
March 2021
February 2021
January 2021
Author
I'm Jennifer Pettigrew and, true story, I first became interested in Legal Nurse Consulting after my auto insurance company was sued following a car accident in which I was found to be at fault. I wasn't sued until after the statute of limitations was up but an exception was made and the plaintiff alleged that because of being rear-ended he was on pain medications chronically which caused him to develop diabetes and become blind. As a nurse I knew that Diabetic retinopathy cannot develop over the course of just a few years but rather is a complication that develops after several years of untreated or poorly treated diabetes. The case was settled by the insurance company before ever going to court for several million dollars, but from that point on I have been interested in the difference medical professionals could make in legal proceedings.
Clinically I have participated in the direct patient care of patients suffering from injuries related to car accidents, falls, rape, battery, poisonings, burns, gunshot wounds and major medical problems, and I've worked with patients from newborn through geriatric populations.
Categories |
 RSS Feed
RSS Feed